Approach to Heart Transplant Complications
Cardiovascular
Context
- Cardiac transplantation is a definitive therapy for end-stage heart disease with a worldwide 1 year survival of 85-90%, 5 year survival of ~60% and annual mortality rate of 4%.
- Infection and rejection are the leading causes of mortality in the first year.
- Most common symptoms of complication in heart transplant patients presenting to an emergency department: fever and shortness of breath.
Diagnostic Process
Initial Evaluation:
- Thorough history and physical examination are necessary, with particular attention to timing (when the transplant was performed), reason for the transplant, current medications, other comorbidities and history of prior complications or rejection.
Investigations:
- Appropriate standard laboratory testing includes CBC with differential, renal function, liver function, electrolytes, magnesium, phosphorous, troponin and BNP.
- ECG and echocardiogram recommended for all patients with concerning symptoms.
- Have a low threshold for imaging, including a chest X-ray, CT chest and echocardiogram – especially if infection is suspected.
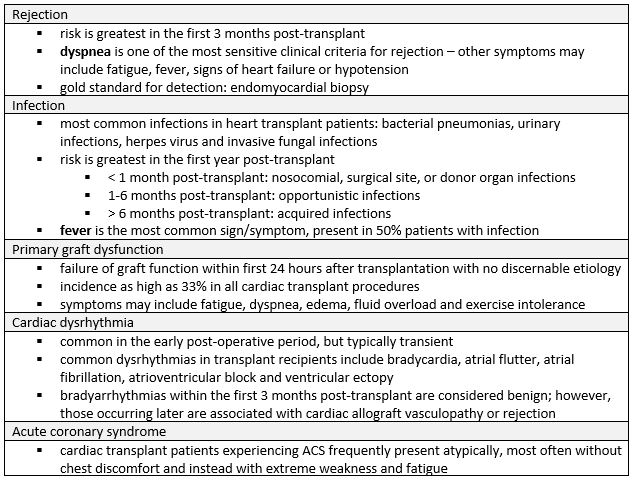
Early Complications:
- Occur in the immediate postoperative period, within days to weeks of the procedure.
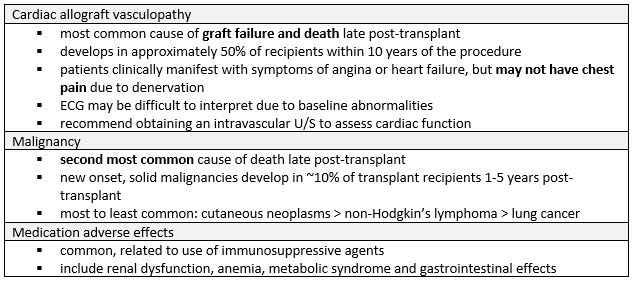
Late complications:
- Occur late in the transplantation period, months to years after the procedure.
Clinical Pitfalls:
- Heart transplant recipients often present atypically without chest discomfort due to cardiac denervation; although reinnervation can occur within 5 years, it is usually incomplete.
- The baseline ECG for transplant recipients will differ from other patient populations; always compare to prior ECGs, if available.
- Resting heart rate in transplant recipients ranges from 80-110 bpm, therefore, bradycardia in this patient population is defined as any heart rate < 80 bpm.
- Other “new baseline” findings may include 2 distinct “p” waves on ECG, right bundle branch block and isolated premature atrial/ventricular complexes.
- Expect troponin and BNP to be elevated for several weeks to 3 months post-transplant, but a new elevation outside of this period can suggest graft rejection, ACS or other acute event.
Recommended Treatment
- Important to take a multidisciplinary approach to care
- Consult early with a cardiologist and/or transplant specialist, if available, to aid with recommendations and considerations.
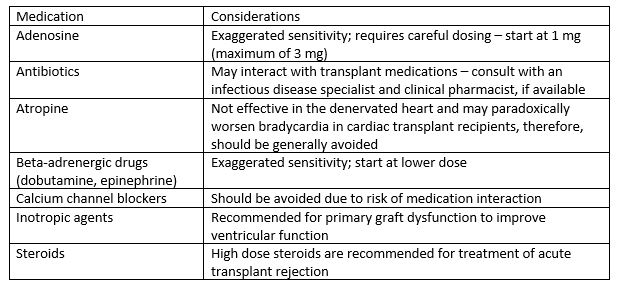
- Pharmacotherapy considerations for heart transplant recipients:
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
These recommendations are based on observational data and expert opinion.
Related Information
Reference List
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated May 06, 2022
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.