Blunt Renal Trauma – Diagnosis & Treatment
Trauma
Context
- Renal trauma can occur in 10-20% of abdominal trauma in adults and children. 1
- Mechanism of injury:
- Blunt trauma 90%2: rapid deceleration or direct force.
- Penetrating trauma 10%.2
- Associated injuries:
- Abdominal injuries, commonly liver or spleen.
- Lower rib fractures.
Diagnostic Process
Clinical Manifestations:3
- Hematuria
- Degree of hematuria does not predict injury severity and may be absent.
- Flank ecchymosis.
- Fractured lower ribs.
Imaging
- When to obtain imaging1:
- Penetrating trauma near the kidney.
- Blunt trauma with:
- gross hematuria.
- microhematuria (>5 RBC per high power field) and hemodynamic instability.
- no hematuria but high index of suspicion based on mechanism.
- Imaging modality1:
- CT abdomen with contrast with delayed urographic phase: allows for grading injury.
- Ultrasound not generally recommended for diagnosis.
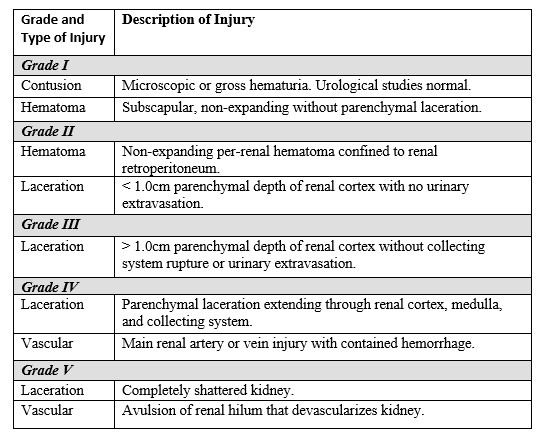
Renal Injury Grading System
Recommended Treatment
- Consult urology.
- If hemodynamically stable
- Blunt trauma
- Initial nonoperative management is recommended for all injury grades.1
- Penetrating trauma
- Initial nonoperative management may be possible for low grade (grade I, II, III) injury with the following1:
- Absence of major blood loss.
- Absence of major renal parenchymal injury.
- Absence of renal vascular injury.
- Absence of associated intra-abdominal injury.
- Initial nonoperative management may be possible for low grade (grade I, II, III) injury with the following1:
- Blunt trauma
- Nonoperative management: observation with supportive care, bed rest, and reimaging as needed.3
- Surgery is recommended for
- Hemodynamically unstable.
- Penetrating injury with active bleeding.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
- High quality evidence for classification of the injury with CT scan with intravenous contrast and delayed urographic phase. 1
Strong recommendation, moderate quality of evidence for nonoperative management for hemodynamically stable or stabilized minor, moderate, and severe lesions. 1
Related Information
Reference List
Coccolini, Federico et al. “Kidney and uro-trauma: WSES-AAST guidelines.” World journal of emergency surgery : WJES 14 54. 2 Dec. 2019, doi:10.1186/s13017-019-0274-x
Voelzke, Bryan B, and Laura Leddy. “The epidemiology of renal trauma.” Translational andrology and urology 3,2 (2014): 143-9. doi:10.3978/j.issn.2223-4683.2014.04.11
Erlich, Tomer, and Noam D Kitrey. “Renal trauma: the current best practice.” Therapeutic advances in urology vol. 10,10 295-303. 10 Jul. 2018, doi:10.1177/1756287218785828
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Jun 20, 2022
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.