Bone Metastases – Diagnosis & Treatment
Hematological / Oncological
Context
The most common site for bone metastases is the vertebra. Although it also occurs in long bones, pelvis, ribs, sternum, and skull.
Complications of bone metastasis are called skeletal-related events (SREs) and include most commonly bone pain, pathologic fractures and hypercalcemia, and less commonly nerve root or spinal cord compression.
Spine Instability Neoplastic Score (SINS) can help determine the need for a surgical referral based on stability of pathologic spinal fractures.
- Breast, prostate, and lung cancer make up near 80% of bone metastases.
- Also kidney, lymphoma, multiple myeloma, thyroid.
- Bone pain attributed to metastases is the principal source of cancer-related pain and can severely impact quality of life.
Clinical Presentation

History
- Cancer diagnosis or features that suggest malignancy if no prior diagnosis (ie: unintentional weight loss, fatigue, drenching night sweats – B Symptoms).
- If cancer diagnosis available:
- Primary cancer.
- Known mets.
- Current treatment (chemo, radiation, next treatment, last treatment).
- Principle oncologist.
- Patients’ Medical Orders for Scope of Treatment (MOST) status.
SREs
-
- Bone pain:
- Typically gradual onset of non-traumatic, dull, aching pain that worsens at night.
- Pathological Fracture:
- Present clinically as a fracture with no history of trauma or only minor trauma.
- Hypercalcemia:
- Renal stones, psychosis, abdominal pain, constipation, polyuria, polydipsia (Stones, bones, abdominal groans, thrones and psychiatric overtones – rarely seen).
- Spinal cord compression:
- Urinary retention, incontinence of stool, weakness in upper or lower limbs, sensory changes in upper or lower limbs.
- Bone pain:
Diagnostic Process
Investigations in the ED
- Imaging: High-risk fracture features for the potential to develop a pathological fracture include painful lesion, >2.5cm in size and >50% of the bone is involved.
- Xray: useful but misses less severe bone metastases.
- CT: more sensitive (74%).
- MRI: 95% sensitivity and 90% specificity for bone metastases and can also detect cord compression (6).
- Specific labs: CBC, Cr/GFR, Calcium, ALP, Serum Protein Electrophoresis (SPEP), UPEP, ECG.
Differential diagnosis
- Benign bone tumor.
- Malignant bone tumor.
- Infection (osteomyelitis).
- Trauma.
- Osteonecrosis.
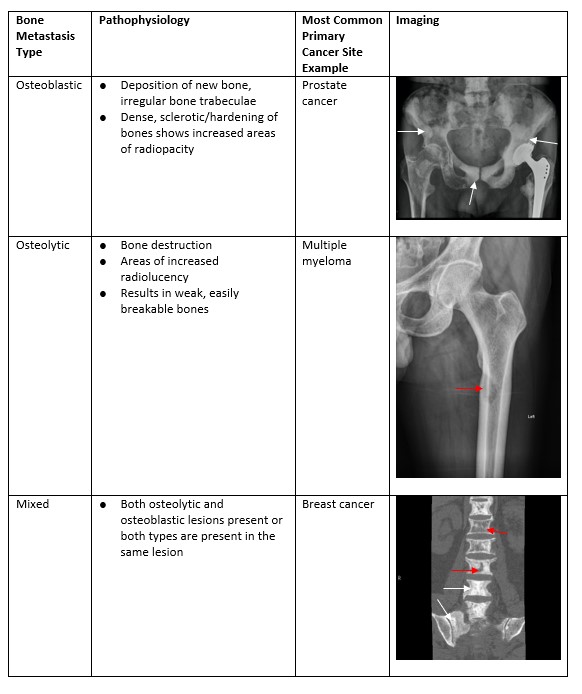
Case courtesy of Dr Mohammad Taghi Niknejad, Radiopaedia.org, rID: 848522
Case courtesy of Dr David Cuete, Radiopaedia.org, rID: 294043
Recommended Treatment
Emergency treatment:
-
Bone pain
- Initial trial with NSAIDs and acetaminophen with step-up to opioids as needed in the setting of acute pathologic fractures and associated pain.
-
Hypercalcemia
- IV fluids are the key.
- Ensure adequate renal function.
- May initiate bisphosphonate therapy in ED if severe hypercalcemia and cardiac instability.
- Alternately zoledronic acid 4mg IV over 15mins or pamidronate 60 – 90 mg IV over 2 hours.
- Moderate asymptomatic hypercalcemia can treated with fluids and calcitonin 4 IU/kg IV.
- Inpatient vs outpatient decision based on:
- Unstable fractures.
- Extent of metastases.
- Spinal cord compromise.
- Referral to specialists (surgery and oncology).
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
There is wide spread agreement in the studies about what is included in skeletal-related events and how they should be managed. There is little variation between studies in the diagnosis and treatment of bone metastases and their complications.
Related Information
Reference List
-
Spinal Instability Neoplastic Score: An Analysis of Reliability and Validity From the Spine Oncology Study Group.
Fourney DR, Frangou EM, Ryken TC, Dipaola CP, Shaffrey CI, Berven SH, et al. 2011 Aug [cited 2021 Apr 10];29(22):3072–7.
J Clin Oncol [Internet]A Novel Classification System for Spinal Instability in Neoplastic Disease From the Spine Oncology Study Group.
Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, et al. (October 15, 2010 – Volume 35 – Issue 22 – p E1221-E1229)
*Combined Neurosurgery and Orthopaedic Spine ProgramManaging skeletal related events resulting from bone metastases.
Wilkinson AN, Viola R, Brundage MD. Vol. 337, 2008. p. 1101–5.
The BMJ.Mechanisms of Bone Metastasis [Internet].
David Roodman G. Vol. 350, 2004 [cited 2019 May 2]
N Engl J Med.Bone metastasis. In: Functional Imaging in Oncology: Clinical Applications – Volume 2 [Internet].
Jayarangaiah A, Kariyanna PT. Springer Berlin Heidelberg; 2014 [cited 2021 Apr 10]. p. 1389–410. NCIB
Relevant Resources
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Jun 01, 2021
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.