Brugada Syndrome – Diagnosis and Treatment
Cardiovascular, Critical Care / Resuscitation
Context
Overview of Brugada syndrome (BrS)
- Inherited heart rhythm disorder that predisposes young patients with a structurally normal heart to malignant ventricular dysrhythmias that results in syncope or sudden cardiac death.1,2
Epidemiology
- 10x more common in men.
- East, and Southeast Asian populations.1
- Responsible for 4-12% of all sudden cardiac deaths.1,2,5
Etiology
- Na+ channelopathies are most common, but Ca2+ and K+ channels are also implicated.
Clinical Manifestations
- 3 clinical presentations:1-5
- Asymptomatic with either a spontaneous or drug induced ECG pattern.
- Syncope, hypoxic seizures, or episodes of nocturnal agonal respirations due to non-sustained ventricular arrythmias.
- Sudden cardiac death (SCD) due to sustained ventricular arrhythmias.
- First arrhythmic events most often occur between the ages of 30-50,1 at night, and/or during periods of rest, increased vagal tone, or sleep.2,5
- ECG changes can be unmasked by fever, ischemia, alcohol, or medications.2,3,5
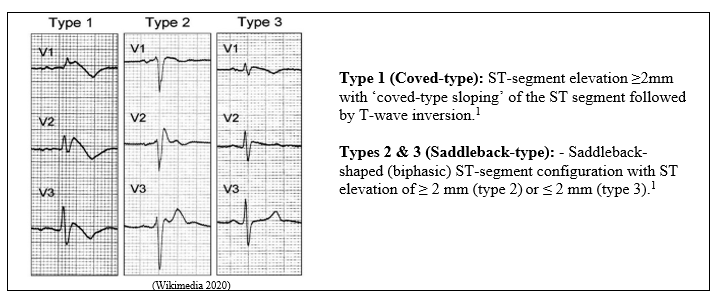
ECG Findings
- Pseudo-right bundle branch block with ST segment elevation in leads V1 to V2.3
- 3 different patterns of ST elevation with J-Point elevation ≥2mm.1
Diagnostic Process
Diagnosis
- RBBB and STEMI are common misdiagnoses. 5
- Diagnosis = Type 1 ECG pattern (Brugada’s Sign) in combination with clinical features1-4 including family history of SCD.3
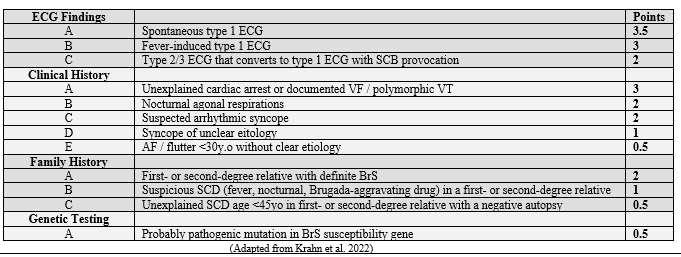
- Recommended diagnostic decision aid is the Shanghai Score which considers ECG findings, clinical history, family history, and genetic testing.1
- Diagnosis:
- probable if ≥ 3.5points;
- possible if 2-3 points;
- nondiagnostic if <2 points.
- Diagnosis:
Differential Diagnosis
- Mmyocardial ischemia.
- Acute pericarditis.
- Pulmonary embolism.
- Right ventricular compression.
- Metabolic disturbances.
Recommended Treatment
Risk Stratification
- Risk assessment is controversial.
- The only definitive factors that increase the risk of a serious arrhythmic event (SAE) are a history of syncope or evidence of a type 1 ECG pattern. 1,2,5
- However, asymptomatic patients and/or patients with an inducible ECG, still demonstrate a concerning 10yr SAE risk. 1,2,5
Management
- Conservative management includes avoidance of known triggers or provoking drugs (see org), prompt treatment of fevers, and limiting alcohol intake. 1,5
- Symptomatic patients are at high risk of a SAE, and the only proven therapy is an ICD.5
- Asymptomatic patients with a drug-induced ECG patternare at low risk of a SAE and ICDs are generally not indicated.5
- Asymptomatic patients with a spontaneous ECG pattern are at intermediate risk and ICD implantation is controvertial.5 Each case requires individual assessment.
- Quinidine is the only pharmacologic agent that has been able to demonstrate prevention of BrS arrhythmias. It is not a first line option due to limited evidence and a large side effect profile.1,5
- Amiodarone is not an effective agent to control BrS arrhythmias. It has been shown to unmask Brugada ECG patterns and aggravate episodes of ventricular fibrillation.6
- Isoproterenol should be used in BrS patients experiencing electrical storms and acute recurrences of ventricular fibrillation (VF).7
Related Information
Reference List
Krahn AD, Behr ER, Hamilton R, Probst V, Laksman Z, Han HC. Brugada Syndrome. JACC Clin Electrophysiol. 2022 Mar;8(3):386-405. doi: 10.1016/j.jacep.2021.12.001. PMID: 35331438.
Brugada J, Campuzano O, Arbelo E, Sarquella-Brugada G, Brugada R. Present Status of Brugada Syndrome: JACC State-of-the-Art Review. J Am Coll Cardiol. 2018 Aug 28;72(9):1046-1059. doi: 10.1016/j.jacc.2018.06.037. PMID: 30139433.
Wylie JV, Garlitski AC. Brugada syndrome: Clinical presentation, diagnosis, and evaluation. In N. Parikh (Ed.), UptoDate, 2021 Accessed April 20, 2021. Available from: https://www.uptodate.com/contents/brugada-syndrome-clinical-presentation-diagnosis-and-evaluation
Coppola G, Corrado E, Curnis A, Maglia G, Oriente D, Mignano A, Brugada P. Update on Brugada Syndrome 2019. Curr Probl Cardiol. 2021 Mar;46(3):100454. doi: 10.1016/j.cpcardiol.2019.100454. Epub 2019 Aug 23. PMID: 31522883.
Gourraud JB, Barc J, Thollet A, Le Marec H, Probst V. Brugada syndrome: Diagnosis, risk stratification and management. Arch Cardiovasc Dis. 2017 Mar;110(3):188-195. doi: 10.1016/j.acvd.2016.09.009. Epub 2017 Jan 27. PMID: 28139454.
Brodie OT, Michowitz Y, Belhassen B. Pharmacological Therapy in Brugada Syndrome. Arrhythm Electrophysiol Rev. 2018 Jun;7(2):135-142. doi: 10.15420/aer.2018.21.2. PMID: 29967687; PMCID: PMC6020192.
Kaneko Y, Horie M, Niwano S, Kusano KF, Takatsuki S, Kurita T, Mitsuhashi T, Nakajima T, Irie T, Hasegawa K, Noda T, Kamakura S, Aizawa Y, Yasuoka R, Torigoe K, Suzuki H, Ohe T, Shimizu A, Fukuda K, Kurabayashi M, Aizawa Y. Electrical storm in patients with brugada syndrome is associated with early repolarization. Circ Arrhythm Electrophysiol. 2014 Dec;7(6):1122-8. doi: 10.1161/CIRCEP.114.001806. Epub 2014 Sep 14. PMID: 25221333.
Wikimedia Commons. File:Brugada.jpg. 2020 Dec. Accessed on Dec 23, 2022.
RESOURCE AUTHOR(S)

DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Feb 13, 2023
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.