Acute Ataxia in Adults (Diagnosis)
Neurological
First 5 Minutes
Red flags 🚩(1-3)
New-onset, hyperacute ataxia (minutes to hours) is a medical emergency → urgent neuroimaging for suspected vascular event.
Other features that point to “Can’t Miss” 🚩etiologies include
- Head trauma
- Meningismus (h/a, fever, photophobia)
- Altered mental status
- Symptoms of elevated ICP (headache, n/v, limb weakness or sensory deficits)
Context
Definition (1-3)
- Irregular timing, precision, amplitude of movements
- Sensory ataxia = proprioception deficits, which could be unrelated to cerebellum (e.g., dorsal column lesions).
- Motor ataxia = distinctly refers to cerebellar deficit.
For acute ataxia in children, see Acute Ataxia in Children (Diagnosis)
Diagnostic Process
Presentation is varied and may only present with one symptom. The commonest ataxic presentations include
- Uncoordinated intentional movements
- Balance issues
- Gait abnormalities (e.g., wide-based gait)
History (1-3)
- Timeline and evolution of symptoms (hyperacute 🚩 vs. acute (<7d) vs. subacute vs. chronic).
- Is this a new problem?
- History of head trauma? 🚩
- Review of systems (e.g., fever, pain, headache, numbness or tingling, peripheral weakness; any changes in vision, hearing, gait, coordination, balance).
- Recent infection.
- Complete medication, drug, ingestion history.
- Family history of movement disorders.
- Past and current medical conditions.
- If balance is the only complaint, ask about vertigo, tinnitus, hearing issues and consider other diagnosis.
- Elevated ICP symptoms (headache, n/v, limb weakness or sensory deficits). 🚩
Physical Exam (1-4)
- Vitals
- Full neurological exam
- Focused cerebellar exam
- Key to look for uncoordinated intentional movements
- Finger/nose test (dysmetria)
- Heel/shin test
- Rapid alternating hand slapping (dysdiadochokinesia)
- Heel tapping
- Hold full glass of water without spilling
- Gait analysis (essential) and tandem walking
- Proprioceptive testing (e.g., Romberg, if positive result B12 deficient)
- Eye movement (nystagmus, opsoclonus) 🚩
- Fundoscopy (papilledema) 🚩
- Reflexes (areflexic) 🚩
- Speech (scanning speech – breaking words/phrases into many syllables)
- Focused cerebellar exam
- Other
- Asterixis (metabolic issues)
- Oscillation of trunk or head
- Neck stiffness (meningismus) 🚩
- Rashes
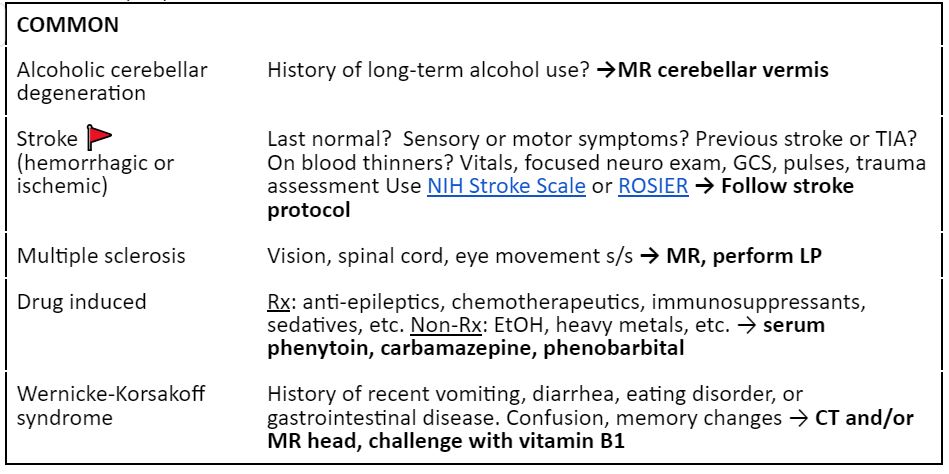
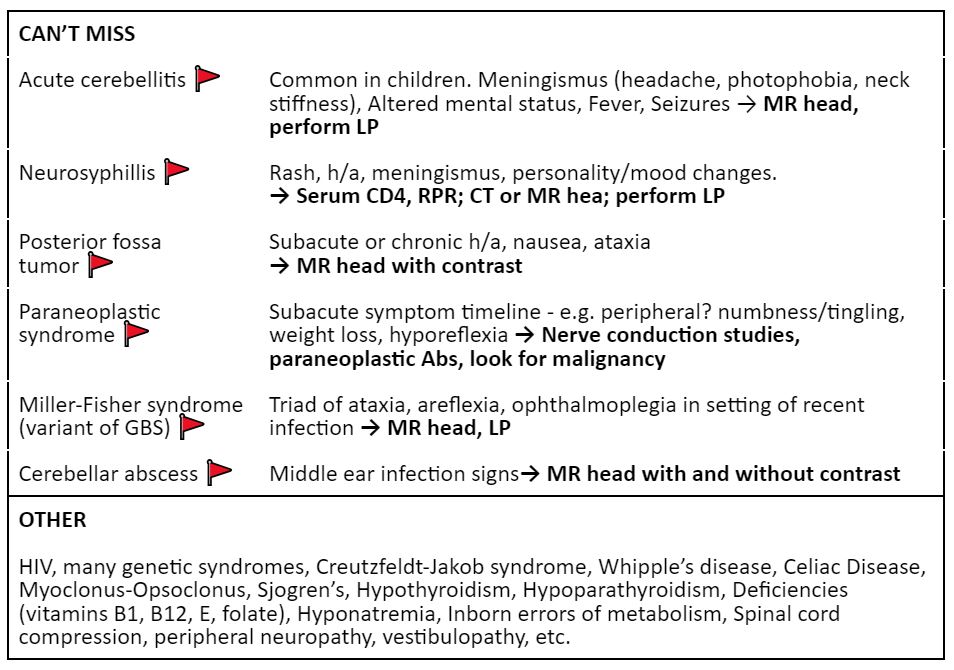
Differential (1-3)
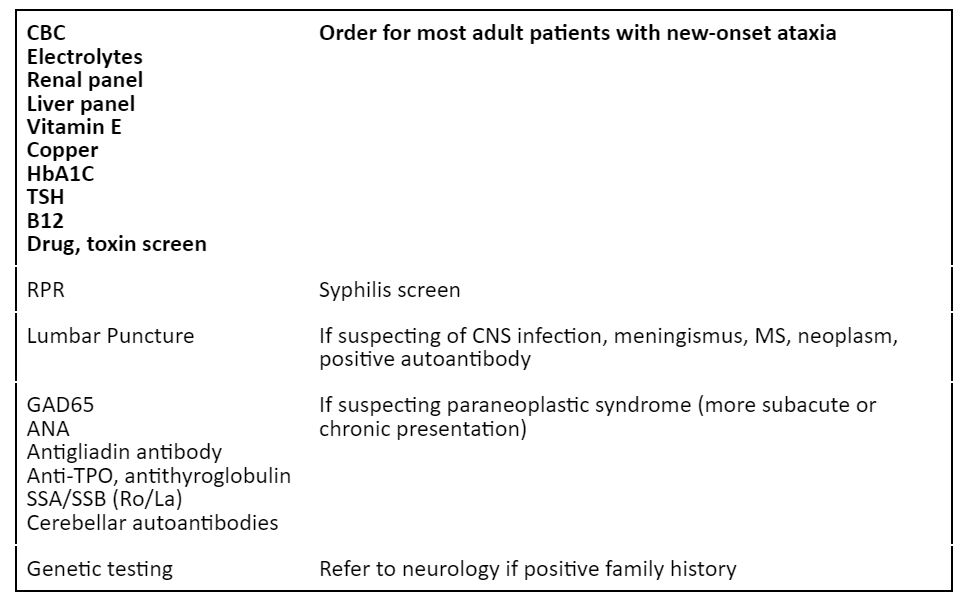
Labs (1,2)
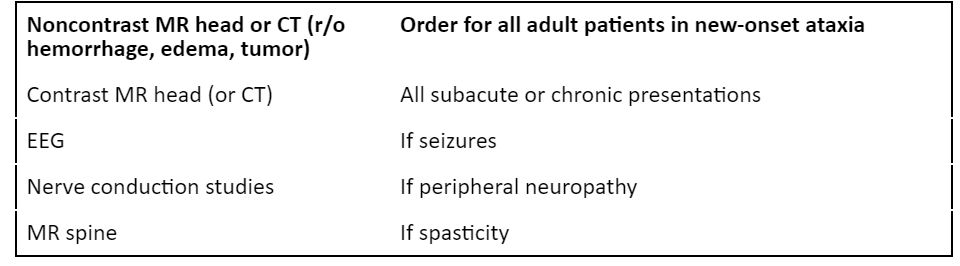
Imaging (1,2)
Recommended Treatment
Management (1-3)
- Stabilize patient.
- Treatment depends on the underlying etiology.
- Many patients with ataxia do not need treatment.
- Refer subacute and chronic cases to neurology.
Criteria For Hospital Admission
- Admit patients with red flag features 🚩
- New, rapid onset ataxia.
- Head trauma.
- Meningismus (h/a, fever, photophobia).
- Altered mental status.
- Symptoms of elevated ICP (headache, n/v, limb weakness or sensory deficits).
- Refer to neurology.
Criteria For Transfer To Another Facility
Stabilized patient.
Comorbidities managed.
Criteria For Safe Discharge Home
- Considerations for discharge
- Patient is stable, not deteriorating.
- Ruled out “can’t miss” etiology with history, physical, labs, neuroimaging.
- Diagnosis identified and/or patient has minimal risk of acutely worsening.
- Consult neurology for unclear presentations and for further investigation of subacute or chronic ataxia.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
Due to variable presentation, broad etiologies, and quality of evidence. No established guidelines for admission or discharge criteria.
Related Information
OTHER RELEVANT INFORMATION
Neurology – Ataxia (Gait) – By Wendy Stewart M.D. – overview of ataxic gait patterns and CNS localization.
Gaits Examination (Stanford Medicine 25) – discusses cerebellar/ataxic gait and Romberg test for proprioceptive deficits.
Reference List
Todd P, Shakkottai V. Overview of cerebellar ataxia in adults. Hurtig H, Eichler A, editors. [Internet]. 2023 [cited 2024 Jan 4]. Available from: https://www.uptodate.com/contents/overview-of-cerebellar-ataxia-in-adults?search=ataxia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
Shakkottai V. Assessment of Ataxia [Internet]. Klockgether T, Perlman S, editors. BMJ Best Practice. BMJ; 2022 [cited 2024 Jan 4]. Available from: https://bestpractice-bmj-com.eu1.proxy.openathens.net/topics/en-gb/1097
Tintinalli JE, O. John Ma, Yealy D, Meckler GD, J. Stephan Stapczynski, Cline DM, et al. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9th edition. McGraw Hill Professional; 2019.
Cerebellum Examination (Stanford Medicine 25) [Internet]. www.youtube.com. [cited 2024 Jan 4]. Available from: https://www.youtube.com/watch?v=Imu1kk_gOKA&ab_channel=StanfordMedicine25
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Feb 14, 2024
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.