Atrioventricular Blocks – First, Second and Third Degree
Cardiovascular
Context
Atrioventricular (AV) block:
- Conduction block between the atrium and ventricles at the level of the AV node and/or Bundle of His.
- First and second-degree AV blocks represent partial impairment of conduction.
- Third degree AV blocks represent complete impairment of conduction.
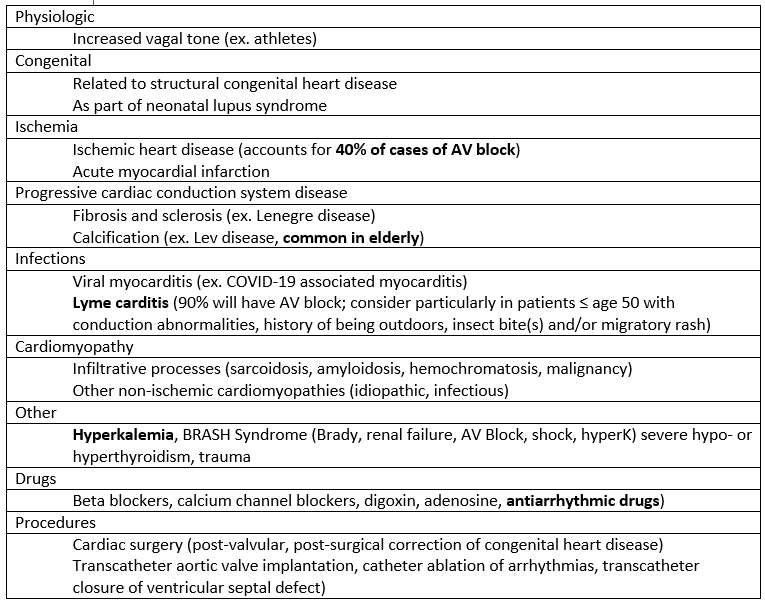
- Top three reversible causes: Drugs, Ischemia, Electrolytes.
Diagnostic Process
Clinical manifestations:
- May be asymptomatic or symptomatic (weakness, dizziness, fatigue, dyspnea, syncope) or manifest as heart failure secondary to bradycardia.
- First degree AV block have higher probability of developing atrial fibrillation.
- Mobitz Type II AV block can progress to third degree AV block and asystole.
- Third degree AV block is a risk factor for asystole and sudden cardiac death.
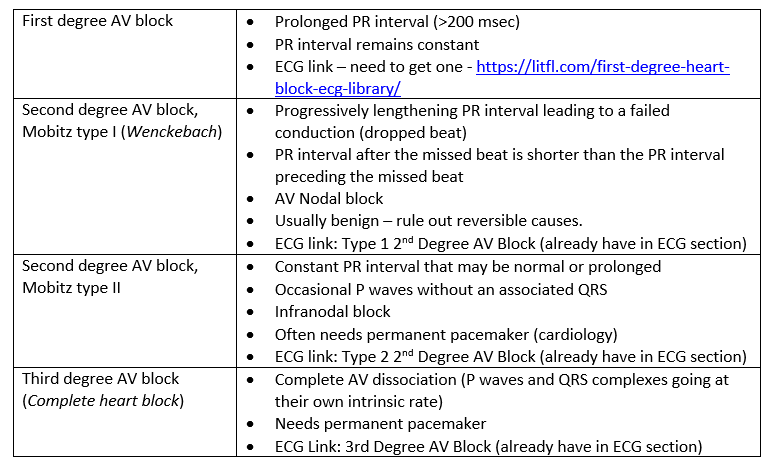
ECG characteristics:
Recommended Treatment
Criteria for admission:
- Newly acquired AV block or symptomatic advanced patients should be admitted to the hospital.
General recommendations:
- Look for reversible causes of AV block.
- Top 3 = Drugs (including overdose); ischemia, and hyperkalemia.
- 4 drugs that typically cause bradycardia in overdose = Calcium channel blockers, Beta blockers, Digoxin and Clonidine.
- Consider also organophosphate exposure, opioids, and amiodarone.
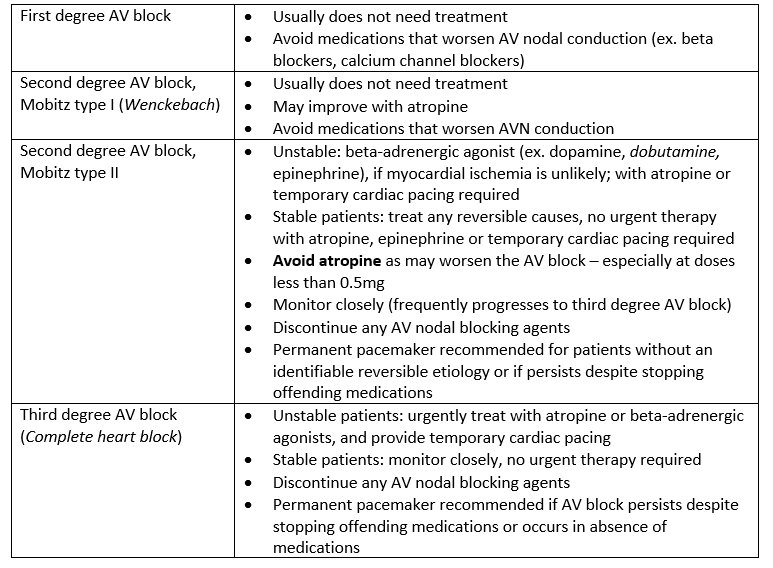
- Treatment summary:
- Markedly symptomatic or hemodynamically unstable patients with second- or third-degree block should be started on drugs/fluids and temporary transcutaneous pacing until a reversible cause is identified or permanent pacemaker is placed.
- Bradycardia Emergency Clinical Summary
Block-specific recommendations:
- Drugs used
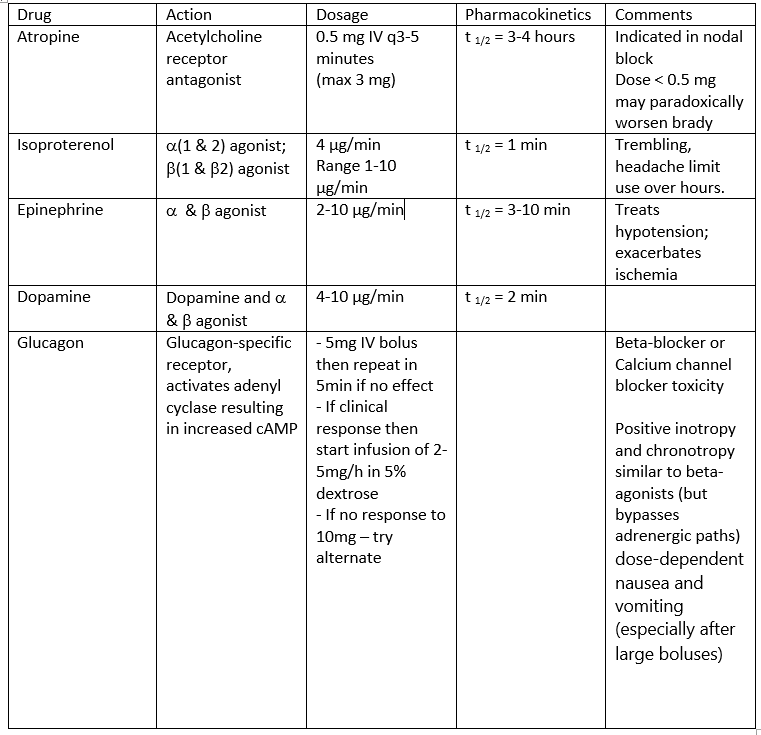
- Specific treatments:
- Digoxin: digibind with poison control guidance.
- Calcium channel blockers: calcium gluconate or chloride, high dose insulin.
- Beta blockers: glucagon 2-10 mg bolus followed by 2-5 mg/hour, high dose insulin.
- Organophosphates: atropine, pralidoxime.
- Opioids: naloxone.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
These recommendations are based on the ACLS guidelines, weak observational data and expert opinion. There is a lack of randomized controlled trials for medications to treat AV blocks.
Related Information
OTHER RELEVANT INFORMATION
Reference List
Walls R., Hockerberger R., & Gausche-Hill M. (eds) Rosen’s Emergency Medicine: Concepts and Clinical Practice. 9th ed. Philadelphia, PA: Elsevier; 2018.
Sauer, W.H. (2022). Etiology of atrioventricular block. UptoDate. Retrieved April 2nd, 2022 from https://www.uptodate.com/contents/etiology-of-atrioventricular-block
Sauer, W.H. (2022). Second-degree atrioventricular block: Mobitz type II. UptoDate. Retrieved April 2nd, 2022 from https://www.uptodate.com/contents/second-degree-atrioventricular-block-mobitz-type-ii
Sauer, W.H. (2022). Third-degree (complete) atrioventricular block. UptoDate. Retrieved April 2nd, 2022 from https://www.uptodate.com/contents/third-degree-complete-atrioventricular-block
Relevant Resources
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Jun 05, 2022
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.