Finger Amputation
Orthopedic, Trauma
First 5 Minutes
Initial Approach to Finger Amputations [1] [2]:
- Address any major arterial hemorrhage first.
- Clean and cover the wound.
- Provide pain management (i.e., digital nerve block or wrist block) [3] [4].
- Preserve the amputated part via cleaning, wrapping in moistened gauze and placing in bag, then place bag in ice water (do not put part in direct contact with ice).
Context
Goals of finger amputation management [5]:
- Preservation of functional length
- Durable coverage
Amputation Description
In the ED setting, simply describing the injury location may be sufficient. To provide additional detail, the below classification may be used for finger amputations distal to the Flexor Digitorum Superficialis (FDS) insertion, it is recommended to distinguish between proximal and distal zones [6]:
Zone 1 Distal Amputations – Fingertip, distal to Flexor Digitorum Profundis (FDP) insertion at root of nail bed.
- Zone 1A – Distal to Lunula, through sterile matrix.
- Zone 1B – Between lunula & root of nail bed, through germinal matrix.
Zone 1 Proximal Amputations – Between FDP and FDS insertions.
- Zone 1C – Between FDP insertion & neck of middle phalanx, periarticular.
- Zone 1D – Between neck of middle phalanx and FDS insertion.
Thumb amputations in this area can be classified using the same method, with the Zone 1 region of the thumb being distal to mid-proximal phalanx of the thumb.
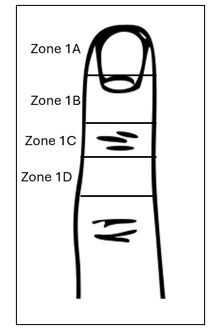
Figure 1. Sebestion and Chung (2011) fingertip amputation zones (Original image modified by Alex Forrester April 18, 2024). File:Hand external anatomy, dorsum.svg – Wikimedia Commons
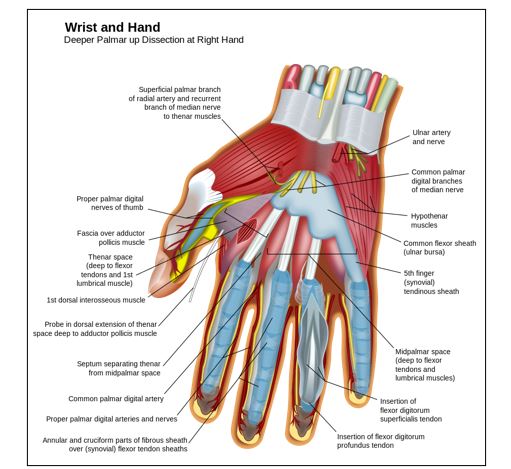
Figure 2. Deep dissection, palmar aspect of hand. Note, insertion of FDS and FDP. File:Wrist and hand deeper palmar dissection-en.svg – Wikimedia Commons
Work Related Amputations
WorkSafe BC (2020) uses the following descriptions for amputations [7]:
- Complete amputation of the digital pulp (thick dense fibrous tissue layer of the fingertip, Figure 3) is equivalent to one quarter of the distal phalanx.
- Amputations of a phalanx or a metacarpal will be assessed by fractions:
- One quarter loss
- One third loss
- One half loss
- Two thirds loss
- Three quarters loss
- Complete loss
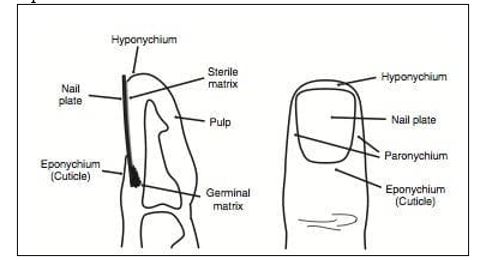
Figure 3. Anatomy of the fingertip. Fingertip Injury • LITFL • Bamboozler
Diagnostic Process
Following patient stabilization: [1] [2]
- Determine extent of amputation.
- Assess for neurovascular complications and crush injuries.
- Determine time of injury.
- Obtain X-Ray.
Recommended Treatment
General management: [1] [2]
- Irrigate stump with saline and control bleeding with direct pressure.
- Preserve the amputated part via cleaning, wrapping in moistened gauze and placing in bag, then place bag in ice water (do not put part in direct contact with ice).
- Provide pain management via digital or wrist nerve block if substantial amputation or multiple lacerations / amputations of fingers [3].
- Tetanus Prophylaxis (if > 5 years since vaccination)[8].
- Antibiotics
- Cefazolin 2 grams IV or;
- Penicillin allergies give Clindamycin 300-450 mg IV / PO or;
- Moxifloxacin 400 mg PO.
- Contact Surgery (usually plastics) OR perform revision / completion amputation procedure in ED.
Revision or Completion Amputation Procedure: [9] [10]
- Perform steps 1 – 5 as shown above.
- Remove nail plate.
- Resect protruding bone to a level that will allow adequate tissue coverage.
- Transect digital nerves proximally as far as possible to avoid painful neuroma development.
- Close skin.
- Repair nail bed and replace nail plate (if possible).
Criteria For Hospital Admission
- Other serious injuries related to trauma.
- Surgery.
Criteria For Transfer To Another Facility
- Surgery required, cannot be performed at current facility.
- Current facility unable to manage patient with other trauma related injuries.
Criteria For Close Observation And/or Consult
Assume that all finger amputations may be reimplanted and consult with the appropriate surgical service (typically plastics) [1] [2] [5].
Surgical Indications:
- Short ischemic time (1 hours warm ≈ 6 hours cold preservation).
- Thumb amputation (loss represents 40-50% function loss).
- Multiple digit amputations.
- Amputations at or proximal to the palm.
- Pediatric finger amputations (any level).
- Single digit amputation distal to FDP insertion.
- Patient occupation functionality requirement.
Criteria For Safe Discharge Home
- If patient proceeds to implantation surgery or terminalization, discharge by admitting service.
- Distal phalanx amputation with controlled bleeding and pain management [2].
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
Finger amputations are fairly obvious to diagnose, and the treatment and management of these injuries in an emergency department setting appears consistent across multiple sources. However, the majority of peer reviewed literature on this subject focuses on the surgical aspect of treatment and not the initial management in the Emergency Department.
Related Information
OTHER RELEVANT INFORMATION
Healthlink BC, Surgery: What to Expect: Surgery: What to Expect | HealthLink BC
Healthlink BC, Post Operation Incision Care: Incision Care After Surgery | HealthLink BC
Emergency Department Discharge Instructions: Finger tip amputation – Sunnybrook Hospital
- Emergency Medicine Cases Podcast, Episode 178: Hand Injuries – Pitfalls in Assessment | Emergency Medicine Cases
- Emergency Medicine Cases Podcast, Episode 179: Hand Injuries – Finger Tip Injuries, Jersey Finger, PIP Dislocations, Metacarpal Fractures, Thumb Injuries, Tendon Lacerations | EM Cases (emergencymedicinecases.com)
- org Traumatic Finger Amputation Case Study: Traumatic finger amputation | Radiology Case | Radiopaedia.org
- An Approach to the Management of an Amputated Digit (youtube.com)
Reference List
C. Nickson, “Life in the Fast Lane – Extremity Injuries,” 3 November 2020. [Online]. Available: https://litfl.com/extremity-injuries/.
J. Swartz, R. Donaldson, S. Rafael, D. Ostermayer, M. Holtz, J. Osgood, N. Young and M. Hwang, “WikEM – Finger Amputation,” 12 December 2020. [Online]. Available: https://wikem.org/wiki/Finger_amputation.
J. Chandrasoma, K. Harrison, H. Ching, L. Vokach-Brodsky and L. Chu, “Peripheral Nerve Blocks for Hand Procedures,” The New England Journal of Medicine, vol. 379, pp. e(15)1 – e(15)5, 6 September 2018.
M. Holtz, R. Donaldson, B. Simpson, Claire, D. Ostermayer and T. Fadial, “WikEM – Nerve Block: Digital Block,” 28 September 2022. [Online]. Available: https://wikem.org/wiki/Nerve_block:_digital_block.
L. Zhang, C. E. Azmat and C. J. Buckley, “Digit Amputation,” 30 January 2023. [Online]. Available: https://www.ncbi.nlm.nih.gov/books/NBK538153/.
S. J. Sebastin and K. C. Chung, “A Systematic Review of the Outcomes of Replantation of Distal Digital Amputation,” Plastic and Reconstructive Surgery, pp. 723-737, September 2011.
W. BC, “WorkSafe BC – Disability Awards – S.195(1) Specifications and Calculations,” 6 April 2020.[Online]. Available: https://www.worksafebc.com/en/resources/law-policy/practice-documents/disability-awards-s195-1-specifications-and calculations?lang=en&origin=s& returnurl=https%3A%2F%2Fwww.worksafebc.com%2Fen%2Fsearch%23sort%3 DRelevancy%26q%3Dfinger%2520amputation%26f%3Al.
ImmunizeBC, “Tetanus and diptheria (Td) vaccine,” Government of British Columbia, 18 March 2024. [Online]. Available: https://immunizebc.ca/vaccines/tetanus-diphtheria-td#Who%20should%20get%20the%20vaccine. [Accessed 25 April 2024].
N. Golinvaux, J. Maslow, J. Hovis and D. Lee, “Fingertip Injury Management,” Journal of Bone and Joint Surgery, vol. 9, no. 3, p. 30, 2019.
Hand Surgery Resource, “Amputation, Finger,” Hand Surgery Resource, 2024. [Online]. Available: https://www.handsurgeryresource.net/amputation-finger. [Accessed 25 April 2024].
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated May 01, 2024
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.