Commotio Cordis
Cardiovascular, Trauma
Context
- Defined as sudden cardiac death due to a blunt, nonpenetrating anterior precordial impact that results in ventricular fibrillation (VF).
- One of the most common causes of sudden death in young male athletes (mean age is 15, 95% are male), which is likely due to decreased chest wall thickness as well as increased likelihood in participation in activities that may involve trauma to the chest.
- Most commonly occurs in sports with spherical small hard projectiles such as baseball, but has been reported in hockey, lacrosse, softball, and fist fights.
- Almost never caused by pneumatic objects (i.e., soccer/tennis balls).
Diagnostic Process
Diagnostic Criteria:
- History: witnessed immediate collapse after a blunt chest impact.
- ECG: VF after impact and normal ECG at baseline.
- Imaging (Echo/CT): no structural heart disease.
- Physical examination: possible delayed onset chest wall contusion overlying the heart.
Investigations:
- There is no role for radiology in the management of commotio cordis, but it can be used to rule out concomitant injury such as sternal fracture.
- Point of care ultrasound may be helpful in ruling out concomitant injuries such as pneumothorax or pericardial effusion/tamponade.
Diagnostic considerations:
- Commotio cordis is a result of having chest wall impact of a specific speed, at a very specific location, and precisely at the right timing in the cardiac cycle to induce VF. Structural damage is only to the chest wall itself. This is an important point in distinguishing sudden cardiac death from more severe trauma that may cause cardiac contusion or myocardial rupture.
- One should also consider other causes of traumatic arrest, such as tension pneumothorax, cardiac or coronary laceration or tamponade, traumatic valvular injury, pulmonary laceration, great vessel injury, hemorrhagic shock, etc., or extrathoracic injuries, depending on the mechanism of injury.
Recommended Treatment
Management:
- Based on standard basic and advanced life support algorithms.
- Focus is on resuscitation from cardiac arrest due to ventricular fibrillation.
- Involves CPR and early defibrillation, with potential role for rescue ventilation or epinephrine should the arrest be prolonged.
- If an AED is not immediately available and the patient is completely unresponsive with no pulse, a precordial thump (impacting the bottom third of the sternum with the ulnar aspect of a clenched fist from ~20cm height), can be attempted, but should not delay defibrillation or CPR.
Prognosis
- In the past, the mortality associated with commotio cordis was reported to be low, with no survivors in the first reported 25 cases. However, more recent cases between 2006-2012 report a 58% survival likely due to earlier recognition, CPR, defibrillation, and activation of emergency medical services
Follow-up and return to activity
- Survivors of commotio cordis should have comprehensive cardiac assessment to exclude underlying heart disease (i.e. channelopathies, cardiomyopathies, catecholaminergic polymorphic ventricular tachycardia) – this includes 12-lead ECG, ambulatory ECG monitoring, echocardiogram, cardiac MRI, and exercise stress test.
- If this workup for cardiac pathology is unremarkable, the patient may return to training and competitions
- Of note, chest wall protectors have not shown to prevent commotio cordis
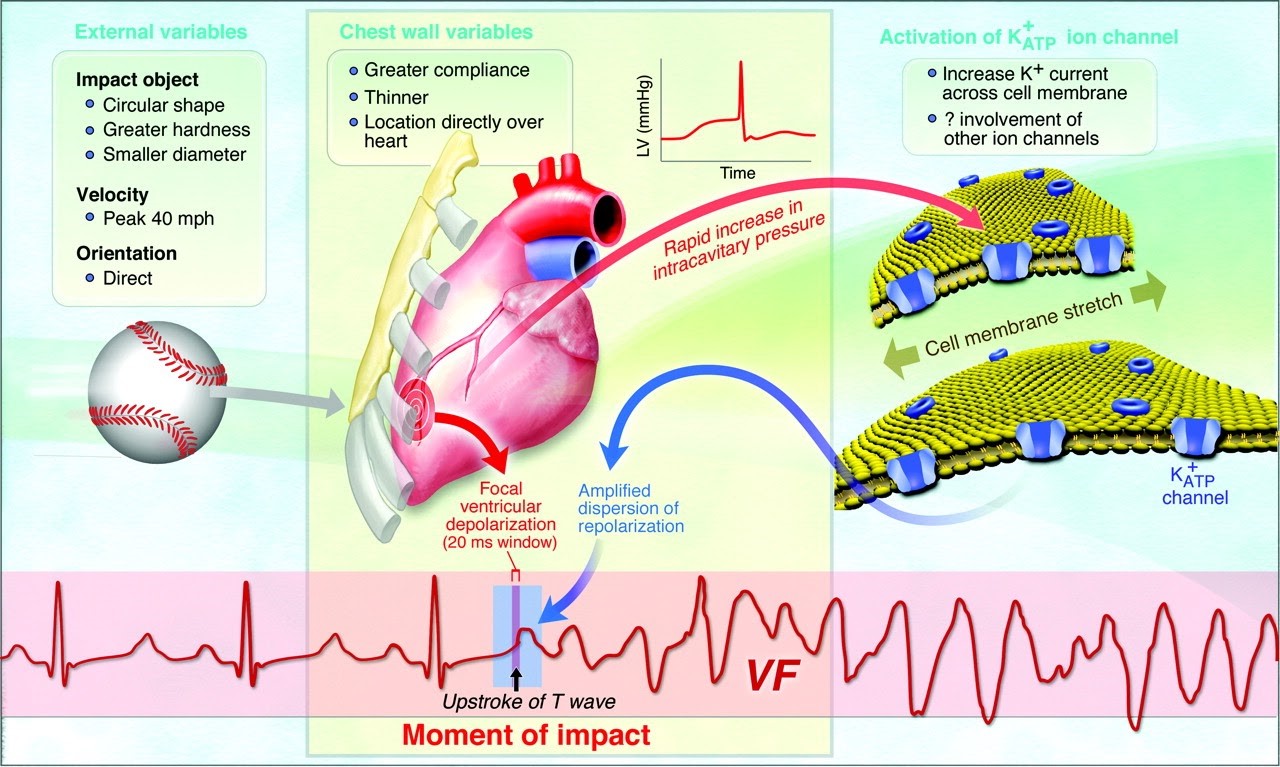
Figure 1: Taken from the American Heart Association (2012)
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
The American Heart Association (AHA) and the American College of Cardiology (ACC) provide strong evidence that commotio cordis survivors should have comprehensive evaluation for underlying cardiac pathology and susceptibility to arrhythmia.
Related Information
Reference List
Walls, R.M., Hockberger, R.S., & Gausche-Hill, M. (2018). Rosen’s Emergency medicine: concepts and clinical practice (9th ed.). Elsevier.
Madias, C. (2021). Commotio Cordis. UpToDate. Retrieved on November 22, 2021 from https://www.uptodate.com/contents/commotio-cordis
Tainter, C. R., & Hughes, P. G. (2021). Commotio Cordis. In StatPearls. StatPearls Publishing.
Horeczko, T. & Inaba, A.S. (2018). Cardiac Disorders. In Rosen’s Emergency medicine: concepts and clinical practice (9th ed., pp. 2099-2125). Elsevier.
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Jan 25, 2022
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.