Difficult Airway Identification in the Emergency Department
Critical Care / Resuscitation, Respiratory
Context
Note: for management see: Difficult Airway Management
- Resuscitative airway management in the emergency department (ED) in the adult population (>16 years of age) is a relatively rare but complex and challenging scenario that includes overdose, trauma, sepsis, airway obstruction, respiratory failure amongst others.
- By definition, the difficult airway includes difficulty with:
- Bag mask ventilation (BMV; oxygenation and ventilation);
- Supraglottic device ventilation/oxygenation; and/or
- Laryngoscopy and intubation
- It is reasonable to assume that every ED airway intervention is difficult until proven otherwise and to be generally prepared for a difficult airway challenge.
- It is possible to predict a difficult airway and to risk stratify patients undergoing procedural sedation who may need airway management during the sedation intervention.
- However, no difficult airway prediction tool is robust and all have suboptimal test characteristics; be prepared!
Management
The Difficult Airway in the ED may be inferred by asking three questions:
- Is the patient potentially difficult to BMV?
- Predicts whether pre-oxygenation or rescue oxygenation will be easy or difficult.
- Any positive component of “BOOTS” (“bearded, older, obese, toothless and/or snoring”) independently predicts potential difficulty with BMV.
- Is the patient potentially difficult to intubate?
- “MMAP”: Mallampati class, Measurement (“3-3-1 rule”), Atlanto-occipital extension, Pathology
Mallampati classification (Class 1 to IV), with mouth opening and extruding tongue in a cooperative patient without phonation is a predictor of difficulty of intubation (Roughly Class 1 = “easy” and Class IV = “difficult). Atlanto-occipital extension: In the absence of Cspine precautions, the patient’s ability to flex the neck at the cervico-thoracic junction and extend the head at the atlanto-axial junction is a predictor of intubation. Pathology means pathologic processes at the periglottic inlet/area including both medical pathology (angioedema, infection, tumors etc) or trauma pathology (blunt or penetrating) and predicts potential considerable difficulty with intubation.
- (Other mnemonics exist such as “LEMON”: Look externally, Evaluate 3-3-2 rule, Mallampati score, Obstruction, Neck Mobility).
- Is the patient potentially difficult to “rescue” with a supraglottic device or difficult to perform a surgical airway on?
The associated mnemonic for difficult “rescue” question (with supraglottic device) is: RODS: Restricted mouth opening, Obstruction, Distorted airway, Stiff lungs or c-spine.
The associated mnemonic for predicting a difficult surgical airway = SHORT: Surgery, Hematoma, Obesity, Radiation distortion or other deformity, Tumor.
Difficult Airway Algorithm
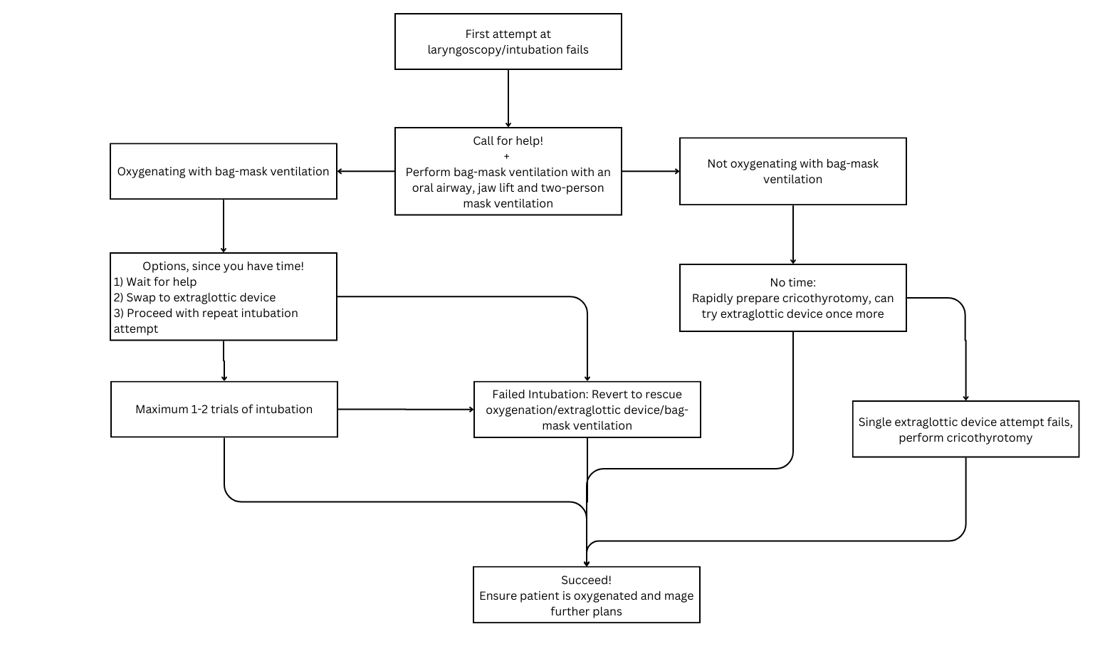
Created By Ella Barrett-Chan, MSI UBC
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
General consensus by airway experts and low-level papers and with predictors possessing low specificity and low positive predictive value.
Related Information
OTHER RELEVANT INFORMATION
The above image of Difficult Airway Algorithm is used with permission. Source:
Henderson JJ, Popat MT, Latto IP, Pearce AC. Difficult Airway Society guidelines for management of the unanticipated difficult intubation. Anaesthesia 2004; 59: 675-94, with permission from Blackwell Publishing Ltd.AIME Airway Interventions and Management in Emergencies – Accessed July 25, 2017.
Difficult Airway Society Guidelines – Accessed July 25, 2017.
Airway Management in Emergencies – Open-access online textbook from www.aimeairway.ca.
Reference List
Relevant Resources
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Oct 31, 2018
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.