Ovarian Cysts – Diagnosis & Treatment
Obstetrics and Gynecology
Context
- Ovarian cysts are found in roughly 35% of premenopausal women and in 17% of postmenopausal women (Pavlik et al 2013).
- Ovarian cysts can be encountered as incidental findings or as symptomatic entities.
- Typically, they are benign. However, they have the potential to represent or to lead to serious pathology.
Pathophysiology
- There are both benign and malignant ovarian tumors. Ovarian cysts are benign tumors originating from one of three cell lines: epithelial, germ cell or sex cord stromal.
- Cysts can be classified as functional/physiologic (eg follicular or corpus luteum) or pathologic. They can be further classified as asymptomatic, symptomatic, hemorrhagic or ruptured.
- Most ovarian cysts are functional as related to normal menstrual cycle:
- Follicular cyst:
- begins when the follicle doesn’t rupture and continues to grow
- often resolve within two or three menstrual cycles
- Corpus luteum cyst:
- fluid accumulates inside the ruptured follicle
- Other benign cysts (not related to menstrual cycle):
- Dermoid cysts or teratomas
- Cystadenomas = benign epithelial neoplasms (cytopathological diagnosis)
- Endometriomas secondary to endometriosis attachment
- The biggest complication of large cysts is the development of ovarian torsion, a true gynecologic emergency.
- Ovarian malignancies are outside the scope of this summary but require consultant management.
- Follicular cyst:
Diagnostic Process
- Ovarian masses can present as asymptomatic incidentalomas or they may present with cyclic or non-cyclic abdominal pain or lower urinary tract symptoms.
- Bloating, early satiety and constitutional symptoms can be associated with ovarian malignancy.
- Physical exam findings are limited, but large ovarian masses can be palpable.
- Ascites and pelvic lymphadenopathy would be more suggestive of malignancy.
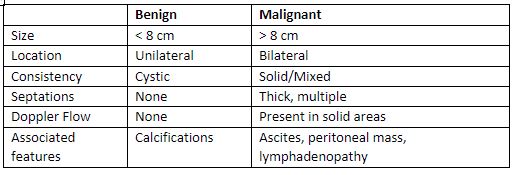
- Ultrasound is the first line in differentiating a benign vs malignant ovarian mass.
- Most benign masses demonstrate typical ultrasound findings (see table 1).
- Ruptured or hemorrhagic cysts will present with acute abdominal/pelvic pain with free fluid in the pelvis and collapsed ovarian cysts on ultrasound.
Recommended Treatment
Treatment recommendations are all adapted from SOGC guidelines/Wolfman et al 2020.
A: Asymptomatic Cysts
- The Society of Obstetricians and Gynecologist of Canada (SOGC) recommends follow-up imaging for asymptomatic ovarian cysts < 10 cm in size based (see figure 1).
- Asymptomatic cysts >10 cm should be referred to an OBGYN due to the risk of possible ovarian torsion and increased risk of malignancy.
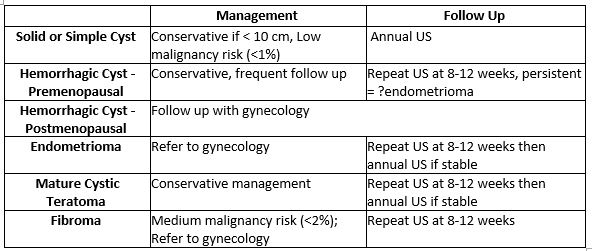
Figure 1: Recommended follow-up for benign, asymptomatic ovarian masses. Image from SOGC guidelines/Wolfman et al 2020.
B: Symptomatic Cysts
- Symptomatic, non-ruptured, cysts should be observed for persistence of symptoms as cysts often resolve on their own with expectant management.
- Avoid definitive intervention for functional cysts (ie physiologic cysts involved with menstrual cycle, such as follicular or corpus luteum cysts).
- NSAIDs should be first line analgesia and there is no role for hormonal management as this has no advantage compared to expectant management alone.
- Should consider referral for cystectomy for symptoms that persist.
C: Ruptured or Hemorrhagic Cysts
- Usually also managed expectantly with NSAIDs for analgesia.
- Admission for hemodynamic instability, uncontrolled pain, or diagnostic uncertainty.
- Obtain baseline labs, including hemoglobin, regardless of disposition.
- Indications for surgical intervention include: hemodynamic instability, increasing hemoperitoneum or declining hemoglobin, symptoms that persist >48 hours or diagnostic uncertainty, including risk suspicion of ovarian torsion.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
Strong: Investigative and treatment recommendations based on recently updated Canadian Clinical Practice Guidelines.
Related Information
Reference List
Relevant Resources
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Oct 06, 2023
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.