Ring Removal
Cardinal Presentations / Presenting Problems
Context
- Ring removal due to ring trauma affects a wide range of patient populations. Ring trauma may develop due to infection, skin disorders, allergic reactions, bee stings, pregnancy, or due to tightness of the ring itself. Penile constriction devices are used to enhance sexual performance and thus affect patient populations engaging in sexual activities.
- Constriction due to rings around any body part (including digits due to wedding bands or penile constriction devices) can lead to necrosis, ischemia, diminished function and amputation.
- Removal of constriction in timely manner will help eliminate ischemia and give the best prognosis for full recovery.
- A number of removal techniques have been described, with none being considered superior over all situations. The best removal technique depends on location on body and patient preference, including desire to preserve the ring (ie in case of wedding band).
Recommended Treatment
Finger/Toe Ring Removal
(Eg: wedding bands). General treatment approach:
- Adequate digital block; bupivacaine or another long-acting anesthetic. Avoid if ischemia findings or wounds/fractures. Avoid epinephrine which can exacerbate ischemia.
- Elevating the arm with application of ice pack for 10-15 min prior to removal can help reduce edema. Inflate a blood pressure cuff around the arm to prevent the redevelopment of this edema.
- Wound management including cleaning and tetanus prophylaxis if needed.
- Ring removal using either ring destructive or ring preserving. Sentimental reasons may mean preservation of ring, tungsten carbide material also poses a problem due to its strength.
Ring Preserving
Begin with these techniques, and if fail, move to ring destructive.
- Two rubber band technique:
Two rubber bands and ordinary liquid soap (lubrication). Rubber bands are then inserted under the ring, use a small artery forceps or similar instrument to help. The rubber bands are looped over the ring and held in separate hands by the clinician, then apply distal traction is with the rubber bands while also oscillating them around the long axis of the digit, through an arc of 180° in alternating directions (similar to turning a wheel on a car). Continue until ring removed.

- Winding technique:
A thread is passed under the ring, then the finger is wrapped proximal to distal direction, and compression should always pass the proximal interphalangeal (PIP) joint. Next, pull the proximal end of the thread toward the tip of finger. The thread will start unwind as you pull it and push the ring toward the tip; gradually, the ring will slide over the compressed finger. - Compression technique: (https://www.youtube.com/watch?v=DrDROoJAF4I)
Need two penrose drains. From Kalken et al (2013): “The principle of this technique is reducing the edema in distal part of finger and blocking the blood flow to congest the finger again. First penrose drain is tightly wrapped around the finger like a tourniquet just distal to the ring and PIP joint and secured in place with the help of a surgical clamp. Second penrose drain is a wound around the finger from the first penrose drain toward the incarcerated ring to compress the edema. While the first penrose drain (tourniquet) is in place, remove the second penrose drain and move the ring over the finger.” - Caterpillar technique:
Not suitable with elderly patients or those with arthritis in PIP joint. Only need lubricant. Wiggle ring over finger (see image if needed).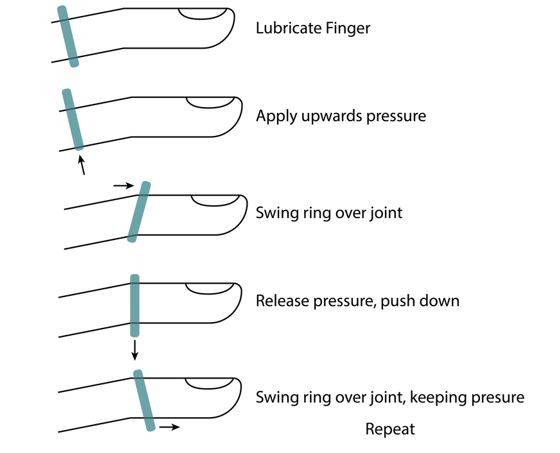
- Twin threads technique:
Not for patients with excessively swollen fingers, open wound, or finger fractures. From Kalken et al. (2013): “Two threads and a lubricant are required in this technique. Any thin and strong thread will work fine; however, surgical sutures can also be used because they are available in most ED. Threads are attached to the ring on the opposite sides. The finger is well lubricated first. The threads must be parallel to the finger and to each other. An assistant takes the threads continuously toward the tip of finger and puts a moderate amount of tension on the threads. The physician holds the ring with the thumb and index fingers from dorsal and volar aspects. First, a controlled outward pressure is applied to the ring on the volar aspect with the thumb; once the ring slowly advanced, the index finger applies the outward pressure. Continuous tension on the threads will prevent the ring to turn back to its place, and the ring will gradually move toward the tip of finger with these alternating movements.”
Ring Destructive Methods
- Manual ring cutters:
For rings made of soft materials such as gold, silver, copper, or plastic. Can also use a large Kelly clamp for a firm grip on the ring without deforming it or introducing anything between the ring and the finger to obstruct removal. Controlled crushing technique using a pair of locking pliers (Allen et al., 2012). - Electric hand saws: (https://www.youtube.com/watch?v=JRpR4wCfE7I)
For rings made of steel, tungsten carbide, or titanium. Electric saws, Dremel motor saws, diamond-tipped saws, dental saws, or dental drills can be used for these types of rings. Keep finger wet to avoid friction-associated heat and burns. Placement of a tongue depressor under ring if possible will minimize burn risk.
Penile Ring Removal
- ‘Queen Elizabeth Tuck Technique’:
A penile block using 1% Lidocaine, as well as multiple doses of IV Fentanyl can be administered for analgesic control. This is a two-person technique involving the insertion of 2 large Penrose drains on either side of the penis – between the device and the skin. Lubrication should be liberally applied. Both ends of the drain were gripped firmly in one hand of each operator providing constant traction at 90 degrees to the device. One operator then uses their contra-lateral hand to shimmy the device distally. Simultaneously, the oedematous skin is ‘tucked’ beneath the device by the second operator using their contra-lateral hand. - Electric ring cutter or bolt cutters.
- Electric grinder:
Treat pain with morphine, but do not sedate patient as need to be able to communicate any sensations of pain or heat during procedure. Slip laryngoscope blade (can you use a tongue depressor?) under ring to protect skin. Drape surrounding area. Frequently irrigate genitals and area with ice water to avoid burns. Using Makita angle grinder, grind the ring off. Ensure frequent cooling and irrigation.

Advised against:
- For penile rings, avoid the use of the diamond tip saw as this may lead to major vascular or soft tissue injury of the penis.
Criteria For Close Observation And/or Consult
Follow up regarding sensation and functioning is recommended for cases in which ischemia and/or severe swelling was present.
Related Information
Reference List
RESOURCE AUTHOR(S)

DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Oct 25, 2020
Visit our website at https://emergencycarebc.ca
COMMENTS (2)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.