Tendinopathy – Diagnosis & Treatment
Orthopedic
Context
- Formerly known as “tendinitis”, tendinopathy is now an umbrella term that encompasses tendinitis, tendinosis and tenosynovitis.
- Tendinopathy is a clinical syndrome characterized by chronic pain and decreased function, usually due to repeated mechanical loading (known as overuse) with non-inflammatory changes in the tendon from healing.
- Commonly involved sites include the rotator cuff, elbow, first dorsal compartment of the wrist, hip, knee, and ankle.
- A wide variety of patients with tendinopathies may present to the emergency department due to overuse, and increased participation in athletic activities and activity in younger individuals.
Diagnostic Process
History:
- Determine if there are risk factors present:
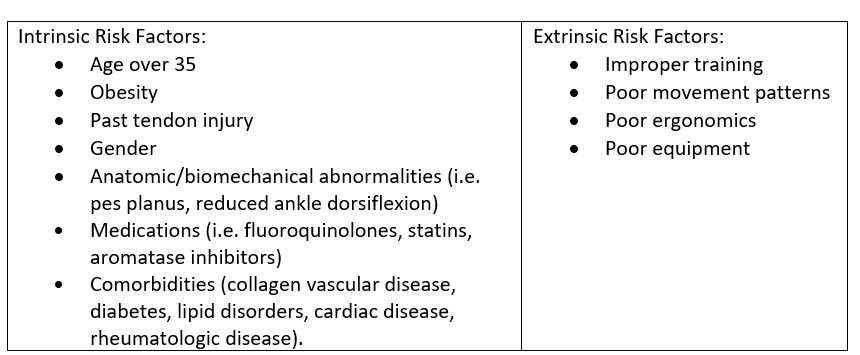
- Ask about recent changes to activity, equipment, or medications.
- Almost all patients with tendinopathy present with pain.
- Latency is a common pattern in tendinopathies. It is a short-lived increase in pain during initial loading of the tendon, followed by a decrease in pain as the exercise continues. However, the pain is worse than baseline a few hours after exercise or the next day.
Physical Examination:
- A thorough MSK examination should be performed in the affected region including passive/active range of motion, joint stability and strength.
- Palpation of the tendon, noting crepitus or warmth, is important. In more superficial tendons, tendon thickening may be appreciated.
- Assessing for signs of edema, effusion, erythema, atrophy, deformity, asymmetry, or trauma can be helpful.
- Physician should attempt to reproduce the patient’s pain.
Investigations:
- Although the diagnosis is usually made on clinical grounds, outpatient ultrasound or MRI can be useful in confirming the diagnosis of tendinopathy.
- Plain radiographs may be ordered to rule out suspected bone abnormalities.
- Laboratory exams are not usually indicated unless tendinopathy is in multiple sites or without apparent overuse etiology. In these cases, metabolic risk factors (A1C, lipids, uric acid) and inflammatory markers (RF, ESR, CRP) can be ordered.
Diagnostic considerations:
- The differential diagnosis for tendinopathy includes tendon rupture, ligamentous injury, arthritis (inflammatory, osteoarthritis), fracture, tumors, osteochondritis, bursitis, septic arthritis, foreign body, osteomyelitis, nerve entrapment syndromes, and tendon sheath infections.
Recommended Treatment
Management:
- In all cases, it is important to ensure that the patient has been referred for appropriate follow-up care with a physiotherapist or an exercise specialist for rehabilitation, which is the most important component of treatment.
- Identification and cessation of the cause of the pain and optimization of extrinsic risk factors should be discussed with the patient.
- Short-term therapies:
- Application of ice, relative rest (+/- splinting), compression, and elevation can be helpful.
- NSAIDs (oral or topical) can be used for analgesia (5-7 days).
- Corticosteroid injections may be helpful, but may lead to higher risk of relapse (Do NOT inject corticosteroids into major tendons such as the patellar or Achilles tendons).
- Nitroglycerin patches have been shown to be helpful in some cases (rotator cuff, Achilles) and may be used off-label, if the patient has failed conservative measures or in conjunction with physiotherapy. These should ideally be done in follow-up with a sports medicine specialist.
Disposition:
- Most patients can be discharged home with proper discharge instructions and appropriate follow-up.
- Set patient expectations that tendinopathies can take weeks to months to resolve.
- Early consultation with a sports medicine physician can be beneficial for athletes and other patients with sports-related tendinopathy for diagnostic and treatment recommendations.
- Exceptions to this would be the elderly and disabled patients, who may have difficulty with activities of daily living due to their tendinopathy.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
Multiple controlled trials support the use of topical NSAIDs for short-term pain control.
Evidence for nitroglycerin patches is drawn from 2 small randomized trials from the same research group.
Related Information
Reference List
Scott, A. & Rees, J. (2021). Overview of overuse (persistent) tendinopathy. UptoDate. Retrieved December 15, 2021 from https://www.uptodate.com/contents/overview-of-overuse-persistent-tendinopathy
Geiderman, J.M. & Katz, D. (2018). Tendinitis and tendinosis. In Rosen’s emergency medicine: concepts and clinical practice (9th ed., pp. 445-463). Elsevier.
Hogrefe, C. & Martin Jones, E. (2018). Tendinopathy and bursitis. In Rosen’s emergency medicine: concepts and clinical practice (9th ed., pp. 1392-1401). Elsevier.
Tendinopathy. (2021, December 15). In ClinicalKey for University of British Columbia [Clinical Overview]. https://www.clinicalkey.com/#!/content/clinical_overview/67-s2.0-6a7e7e17-5cde-41cc-beaf-3bc48f0aeacf
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Feb 17, 2022
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.