Renal Colic – Treatment
Urological
Context
- Urolithiasis accounts for a significant proportion of emergency department visits every year.
- The severity of symptoms, as well as the degree of intervention required is variable.
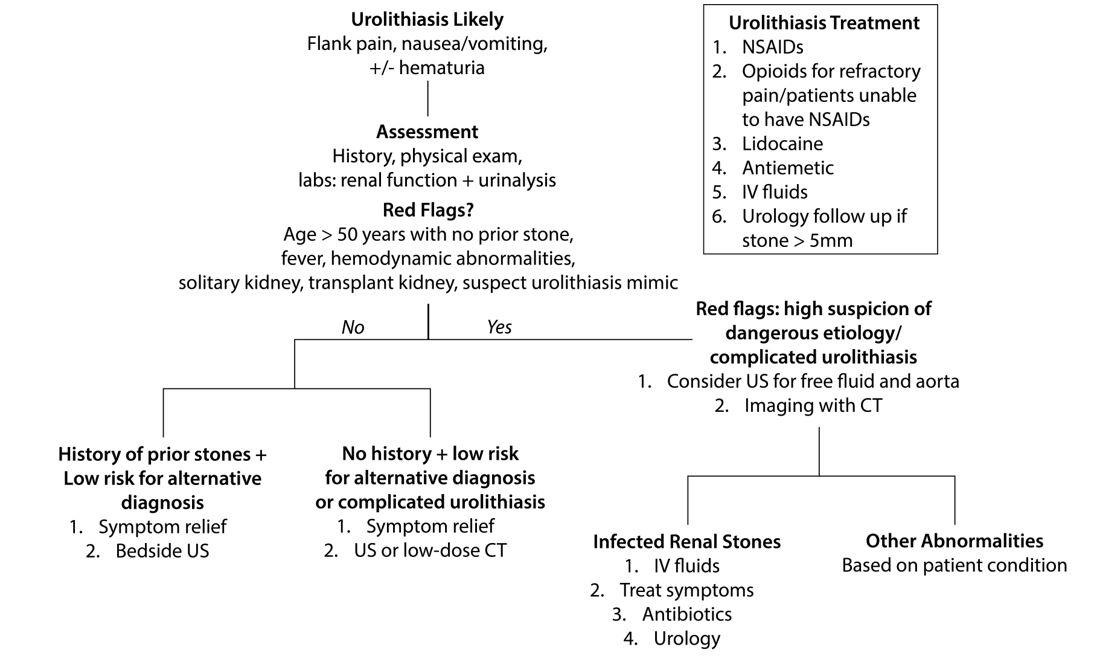
Complicating Factors
- Infection.
- Solitary or transplanted kidney.
- Moderate to severe acute kidney injury.
- Anuria.
- Immunosuppressed.
- Extremes of age.
General Treatment Principles
- Symptomatic treatment for pain and nausea/vomiting should be initiated quickly in patients with suspected urolithiasis.
- Analgesia:
- NSAIDs are recommended as first line treatment.
- Should be avoided in patients with known moderate to severe CKD (GFR < 30) or patients at risk for severe hypovolemia.
- Ketorolac 15 – 30 mg IV.
- Indomethacin 100 mg suppository.
- Opioids are often required in cases of refractory pain.
- Should be avoided in patients with known moderate to severe CKD (GFR < 30) or patients at risk for severe hypovolemia.
- Medical expulsive therapy (MET):
- Tamsulosin is generally recommended for stones 5-10 mm in size.
- Dose = 0.4 mg po daily.
- Use of other agents for MET is not routinely recommended (ex. Nifedipine, Tadalafil).
- There is no evidence that intravenous fluids facilitate faster stone passage and thus should only be used for management of fluid status (significant vomiting or dehydration).
- Tamsulosin is generally recommended for stones 5-10 mm in size.
- Infection:
- Should be treated rapidly with cultures followed by antibiotics.
- Hemodynamically stable:
- Ceftriaxone 1-2 g IV q24h.
- gentamicin 6 mg/kg IV (ideal body weight) and not it CrCl < 30 ml/min.
- Hemodynamically unstable:
- Meropenem 1 g IV q8h + Vancomycin 15 mg/kg IV q12h (consult Inf Disease/ Internal Med).
- Hemodynamically stable:
- Should be treated rapidly with cultures followed by antibiotics.
- NSAIDs are recommended as first line treatment.
Clinical Course
- Rates of spontaneous passage are related to size and location.
- Size:
- Majority of stones < 5 mm will pass spontaneously within 4 weeks.
- 5 – 7 mm stone = 60% passage rate.
- 7 – 9 mm stone = 48% passage rate.
- > 9 mm = 25% passage rate.
- Location:
- Proximal ureter (above SI joint) = 48% passage rate.
- Mid ureter (at SI joint) = 60% passage rate.
- Distal ureter (below SI joint) = 75% passage rate.
Indications for Surgical Consultation
- Septic stone is a urological emergency and warrants urgent consultation.
- Acute kidney injury or anuria.
- High grade obstruction of solitary or transplanted kidney.
- Stone size > 10 mm.
- Stone 5 – 10 mm causing obstruction/hydronephrosis.
- Intractable pain or vomiting.
Indications for Hospital Admission
- Complicated urolithiasis.
- Unable to achieve adequate symptom control for discharge home.
Disposition Home
- Patients can be safely discharged home if:
- Urolithiasis is uncomplicated.
- Non-toxic appearing.
- Adequate symptom control.
- Tolerating oral intake.
- Stones > 5 mm should be referred to urology for outpatient follow up.
- Provide patient with strainer to obtain any stones for analysis which can help to guide preventative treatment by their primary care provider.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
Evidence for NSAIDs as first line treatment option, with use of opioids for refractory pain is high.
- Evidence for use of tamsulosin for medical expulsive therapy is moderate.
- There have been some conflicting studies regarding proven benefit of Tamsulosin, however it is generally recommended given the relatively low side effect profile and risk of adverse event.
- Evidence for recommendation of surgical consultation and disposition plan is low.
- These recommendations are generally agreed upon, but tend to vary by site.
Related Information
Reference List
Relevant Resources
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Nov 12, 2020
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.