Rib Fractures – Uncomplicated
Respiratory, Trauma
Context
- The most common mechanism associated with rib fracture is blunt trauma (1).
- Non traumatic causes secondary to cancer and osteoporosis will not be reviewed here.
- Diagnosis is frequently made on Chest Xray, but CT may be considered if suspicious for underlying injuries or in elderly populations.
- NEXUS CT Chest rule can provide some guidance on when to image in trauma cases.
- Ultrasound/PoCUS can be an alternative to Chest Xray if the user is proficient in its use.
- CT remains the gold standard.
- Rib fractures and associated injuries often carry a high mortality. In adults a mortality of up to 10% has been shown and this increases up to 20% in patient populations >65 yo (2,3).
- 1st and 2nd rib fractures may be associated with great vessel injury, whereas fractures to ribs 9-12 can cause splenic, liver or kidney laceration (4).
- Pulmonary complications including pneumothorax, hemothorax, pulmonary contusion, pneumonia and atelectasis are common and may be seen in 16-52% of blunt trauma cases with rib fracture (4).
Typical Course
- The majority of isolated/simple rib fractures <3, non flail segment, no associated injuries will respond to conservative management (1,3).
- Pain can compound an underlying pulmonary contusion leading a patient into Acute Respiratory Distress Syndrome (5).
Pitfalls
- Not recognizing associated injuries either pulmonary (listed above), abdominal solid organ or thoracic great vessels.
- Under-treating pain may lead to respiratory deterioration.
- If there is a high index of suspicion order a CT chest for more definitive characterization of injuries.
Recommended Treatment
Respiratory
- Incentive spirometer (1,5).
- Pulmonary hygiene including chest physiotherapy, pulmonary toilet, cough and deep breath, and early mobilization lack data and evidence but have been included in the most recent Western Trauma Association guidelines (2).
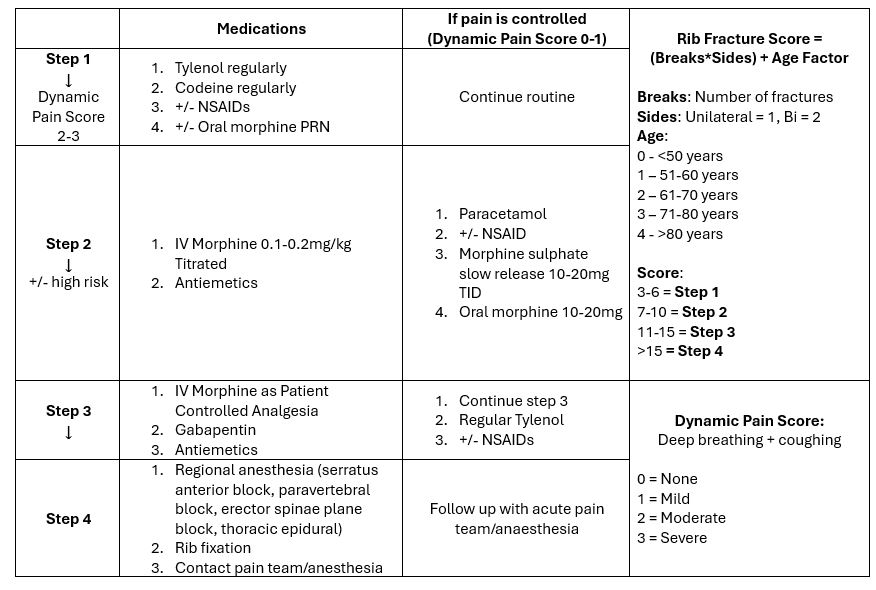
Pain Control (Similar to WHO analgesic ladder)
- Acetaminophen and Ibuprofen (2,5).
- Opiates, start with oral and step up to IV if needed, used in conjunction with either acetaminophen or ibuprofen (3,5).
- Other adjuncts to consider include gabapentin and muscle relaxants although these have limited evidence.
- Some studies have shown benefit of epidural delivered opiates in pain control (3,5). This is more applicable in an inpatient setting.
Regional Anesthesia
- Newer opiate sparing techniques involving regional anesthesia have shown promise but unfortunately there is limited data to support their widespread use at this time (3,5).
- Techniques include the paravertebral block, intercostal block, serratus anterior block, or the erector spinae block.
Criteria For Hospital Admission
Respiratory
- Hypoxemia O2Sat <92% on RA (requiring O2) (3).
- Incentive spirometry <1,000 cc or <15 cc/kg, or a vital capacity of less than 1.4 or 55% of predicted (3).
Age
- Age cutoffs are arbitrary but some institutions recommend admission and observation for >2 rib fractures in patents >65 yo (2).
- Elderly populations are at higher risk for developing complications including pneumonia (5).
Severity
- Flail chest, associated hemothorax, pneumothorax should be admitted and reviewed with trauma service.
- Severe pulmonary contusions will likely exhibit respiratory distress/comprise (as above) and should be admitted.
- Patients with >3 rib fractures, displaced fractures or underlying lung conditions can be considered for admission.
A variety of scoring systems have been developed:
Criteria For Transfer To Another Facility
- If there are severe injuries requiring respiratory support patient may benefit from intubation/ventilation and transfer to ICU/trauma facility.
- Primary transport considerations include ventilation and pain control.
Criteria For Close Observation And/or Consult
- Uncontrolled Pain.
Criteria For Safe Discharge Home
- Adequate pain control.
- Patient able to cough and take deep breath (3).
- No significant underlying injury (see above).
- O2 sat >92% on RA. Ability to perform incentive spirometry >1,000 cc or >15 cc/kg, and a vital capacity of greater than 1.4 or 55% of predicted (3).
- There is limited evidence for follow up chest X-ray in isolated rib fractures, although may consider in higher risk patients.
- Patients may benefit from outpatient follow-up of pain control.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
Limited literature available including landmark papers that are 10-15 years old, and regional trauma guidelines.
Related Information
OTHER RELEVANT INFORMATION
NEXUS Chest CT Decision Instrument for CT Imaging – www.mdcalc.com
Trouble with rib fractures? Learn chest wall blocks (serratus!) with @highland herring. #FOAMed -UltrasoundPodcast.com
Erector Spinae Plane Block – BCpocus.ca
Rib Fractures – JAMA Network Patient Page
Reference List
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Oct 01, 2019
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.