Traumatic Brain Injury Management
Critical Care / Resuscitation, Neurological, Trauma
Context
Traumatic brain injury (TBI) is a major cause of long-term disability in young patients if crucial acute management steps are not taken to prevent additional brain hypoxia. Emerging evidence suggests that optimizing oxygen delivery to the brain in the early hours after the injury can improve long-term outcomes significantly.
Traditionally, TBI has been associated with a fixed injury stemming from the initial insult; however, modification of the final neurological outcome is greatly impacted by resuscitation strategies aimed at preventing secondary ischemic brain injury.
Recommended Treatment
CLICK TO ENLARGE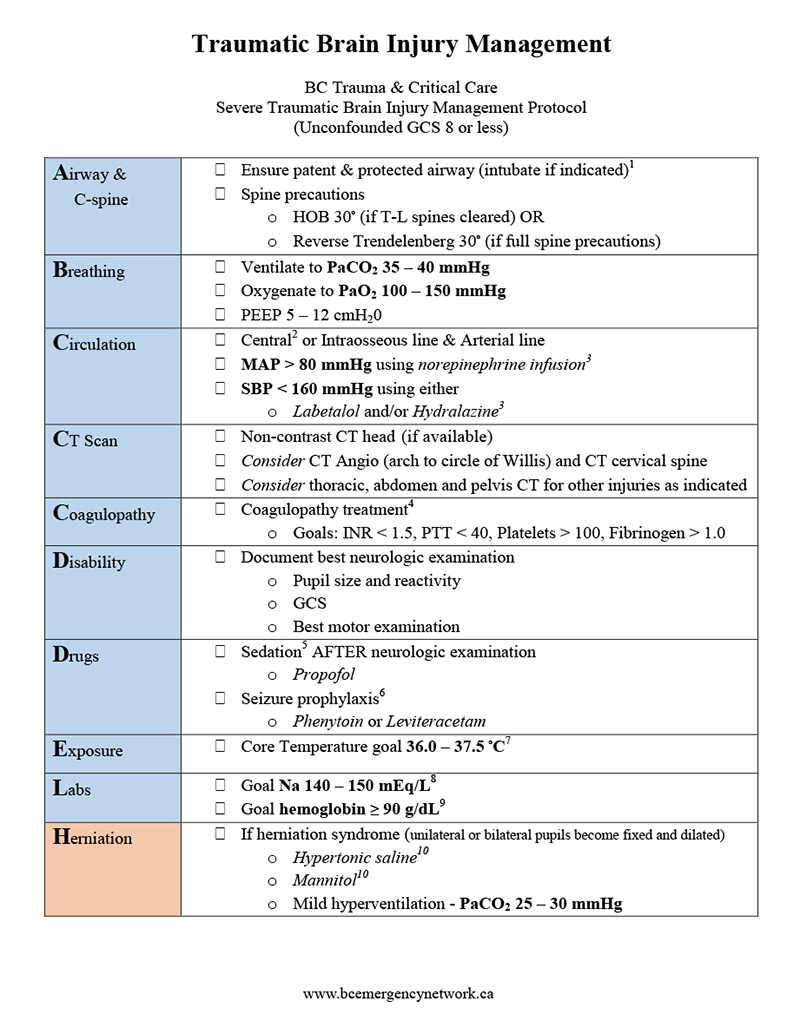
Criteria For Hospital Admission
History of acute traumatic brain injury with an un-confounded Glasgow Coma Score of < 15.
Confounders include:
- Concomitant CNS depressant drug overdose (alcohol, psychotropics, benzodiazepines, opioids and barbiturates)
- Hypothermia (temperature < 34oC)
- Metabolic abnormalities (hypoglycemia, hypo or hypernatremia)
Criteria For Transfer To Another Facility
- Traumatic Brain Injury fulfilling criteria of Canadian CT head rules (Moderate to severe traumatic brain injury (GCS 9-12 = Moderate; GCS < 9 = severe).
- Concomitant TBI with associated multisystem trauma.
Transport considerations
- Consider intubation for all severe TBI patients (GCS < 9) for all ground and air transports.
- Use TBI checklist to optimize cerebral oxygen delivery and prevention of brain hypoxia.
- Transfers should be considered to be life-threatening.
Criteria For Close Observation And/or Consult
History of acute traumatic brain injury with an un-confounded Glasgow Coma Score of < 15.
Criteria For Safe Discharge Home
Not applicable for moderate to severe TBI patients.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
Related Information
OTHER RELEVANT INFORMATION
-
-
Advances in Brain Injury Management – This will blow your mind
UBC Department of Emergency Medicine Grand Rounds – May 9, 2018
Relevant Resources
RESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Nov 26, 2019
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.