Kawasaki’s Disease
Cardiovascular, Inflammatory, Pediatrics
Context
- Kawasaki’s Disease (KD) is one of the most common causes of vasculitis and a leading cause of acquired heart disease in children.
- Boys are affected more commonly than girls.
- 80-90% of cases occur in patients under the age of 5.
- The underlying etiology is unknown.
- Its incidence is highest in Japan at 265 cases per 100,000 children under the age of 5. In the USA, incidence is 20 cases per 100,000 children under the age of 5.
- Usually a self-limiting condition characterized by a prolonged fever with other acute inflammatory manifestations lasting 12 days on average.
- 20-25% of untreated cases develop coronary artery aneurysms, which could lead to myocardial ischemia, infarction, or sudden death. Early recognition and treatment with intravenous immunoglobulin (IVIG) will lower this rate of aneurysms to less than 5%.
- Diagnosis = fever (typically above 38.5ºC) persisting > 5 days AND > 4 of:
- Bilateral non-exudative conjunctival injection, usually limbic-sparing.
- Oral mucous membrane changes (e.g. erythema and/or fissuring of lips, strawberry tongue, and/or erythema of oropharyngeal mucosa).
- Peripheral extremity changes.
- Acute phase: erythema of palms and/or soles and/or edema of hands and/or feet.
- Subacute phase: periungual desquamation.
- Polymorphous rash (maculopapular, diffuse erythroderma, or erythema multiforme-like).
- Cervical lymphadenopathy (at least one lymph node ≥1.5 cm in diameter, usually unilateral).
- Algorithm of evaluating suspected KD below:
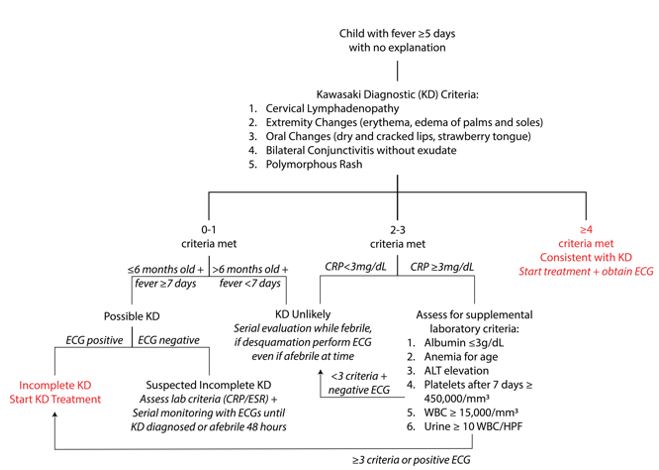
created by Ella Barrett-Chan, MSI UBC
Recommended Treatment
- Immediate treatment includes:
- IVIG 2 grams/kg x 1 dose over 8 to 12 hours.
- High-dose acetylsalicylic acid 30 to 50 mg/kg/day in 4 divided doses up to 4 grams per day until fever resolves, then give low-dose acetylsalicylic acid (local guidelines may differ).
- Consider glucocorticoids 2 mg/kg/day PO or IV in three divided doses for 10 days then 1 mg/kg/day for 5 days if history of IVIG resistance noted (local guidelines may differ).
- Further investigations and treatments listed in algorithm below:
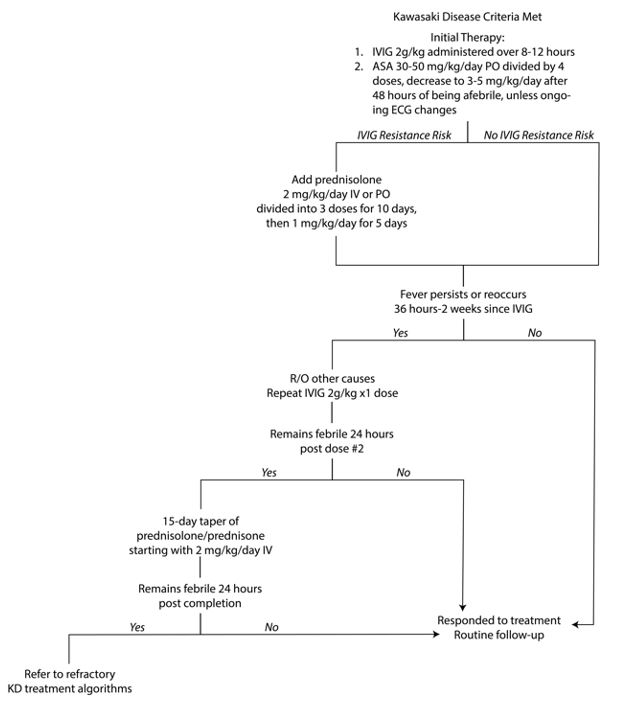
created by Ella Barrett-Chan, MSI UBC
Criteria For Hospital Admission
All patients diagnosed with KD need referral and admission.
Criteria For Transfer To Another Facility
Dependent on local guidelines.
Criteria For Close Observation And/or Consult
Suspicion of KD in a patient warrants consult to pediatrics/internal medicine and cardiology.
Criteria For Safe Discharge Home
Dependent on patient’s clinical response to treatment and echocardiogram results.
Quality Of Evidence?

High
We are highly confident that the true effect lies close to that of the estimate of the effect. There is a wide range of studies included in the analyses with no major limitations, there is little variation between studies, and the summary estimate has a narrow confidence interval.
Moderate
We consider that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. There are only a few studies and some have limitations but not major flaws, there are some variations between studies, or the confidence interval of the summary estimate is wide.
Low
When the true effect may be substantially different from the estimate of the effect. The studies have major flaws, there is important variations between studies, of the confidence interval of the summary estimate is very wide.
Justification
A single dose of intravenous immunoglobulin 2 grams/kg administered over 8 to 12 hours IVIG is most effective if administered within the first 10 days of illness, before aneurysms typically develop.
- Acetylsalicylic acid 30 to 50 mg/kg day provides some anti-inflammatory and anti-platelet effects.
- Glucocorticoids can decrease the rate of coronary aneurysm abnormalities in patients, especially those of Japanese heritage, at high risk for IVIG resistance.
- Postpone administration of live-virus vaccines for at least 11 months in children who have been treated with IVIG because IVIG can interfere with vaccine immunogenicity.
Related Information
Reference List
Relevant Resources
RELEVANT RESEARCH IN BC
Stroke and Transient Ischemic AttacksRESOURCE AUTHOR(S)
DISCLAIMER
The purpose of this document is to provide health care professionals with key facts and recommendations for the diagnosis and treatment of patients in the emergency department. This summary was produced by Emergency Care BC (formerly the BC Emergency Medicine Network) and uses the best available knowledge at the time of publication. However, healthcare professionals should continue to use their own judgment and take into consideration context, resources and other relevant factors. Emergency Care BC is not liable for any damages, claims, liabilities, costs or obligations arising from the use of this document including loss or damages arising from any claims made by a third party. Emergency Care BC also assumes no responsibility or liability for changes made to this document without its consent.
Last Updated Jun 01, 2020
Visit our website at https://emergencycarebc.ca
COMMENTS (0)
Add public comment…
POST COMMENT
We welcome your contribution! If you are a member, log in here. If not, you can still submit a comment but we just need some information.